
.

- The massive increase in shelling against the population of Donbass on February 16 told the Russians that a major offensive was imminent. This is what led Putin to recognize the independence of the Republics and to consider an intervention under Article 51 of the UN Charter.
- Russian President Vladimir Putin launched the full-scale invasion of Ukraine on February 24. Moscow has pleaded "self-defense" under Article 51 of the UN Charter.
- “On 17 February, President Joe Biden announced that Russia would attack Ukraine in the next few days. How did he know this? It is a mystery. But since the 16th, the artillery shelling of the population of Donbas had increased dramatically, as the daily reports of the OSCE observers show.”
- Between 2014 and 2022 the War in Donbas killed an estimated 14,000 people, forcing millions of people to flee the region, and turning the conflict zone into one of the world’s most mine-contaminated areas.
T=1786329678 / Human Date UTC: Monday, 10 August 2026 at 02:41:18
___
OSCE Reports Reveal Ukraine Started Shelling The Donbas Nine Days Before Russia's 'Special Military Operation'
The Biden Administration, U.S. political officials, and the corporate media are lying the American public into World War III.

All of my articles on the Ukraine-Russia War — Part I, Part II, and Part III.
American history is replete with examples of politicians, the corporate media, and the military-industrial complex using lies, false pretenses, and propaganda to sell war to a public that would otherwise be hesitant to send their sons and daughters off to fight on foreign soil.
President Lyndon B. Johnson lied about the Gulf of Tonkin to justify American military intervention in Vietnam.
President George H.W. Bush used a fabricated story of Iraqi soldiers ripping babies out of incubators to start the Gulf War. [Nayirah testimony - Wikipedia]
President George W. Bush lied about “weapons of mass destruction”.
From “Remember the USS Maine”, to the sinking of the Lusitania, to Syrian [False Flag] gas attacks, the last century is filled with example after example of the United States government lying to its citizens in order to justify new wars.
In all of these examples, the corporate press acted as dutiful stenographers of the military-industrial complex hypnotizing the American people with lies, deception, and propaganda.
If the old adage is true that the first causality of war is the truth then it should follow that the first battle between Russia and Ukraine was also won with lies.
It is important to remember that the armed conflict in eastern Ukraine started in 2014 after the Obama administration and U.S. Congress members installed a new government in Ukraine, in what the head of the “private CIA” firm Stratfor called “the most blatant coup in history.”
In response to the U.S.-backed coup, the Luhansk and Donetsk regions in the Donbas held a referendum on seceding from Ukraine, in which 96% of Luhansk and 89% of Donetsk voted for the creation of two new self-described independent republics in eastern Ukraine.
Moscow said the vote reflected the "will of the people," but the European Union called the elections "illegal and illegitimate", which quickly turned violent and descended into an all-out conflict between the Ukrainian military and Russian-backed separatist forces of Luhansk and Donetsk.
Between 2014 and 2022 the War in Donbas killed an estimated 14,000 people, forcing millions of people to flee the region, and turning the conflict zone into one of the world’s most mine-contaminated areas.
The Organization for Security and Cooperation in Europe (OSCE) has had observers on-the-ground monitoring the situation in Donbas since the outbreak of open conflict began in 2014.
The OSCE has been the only international civilian observer mission allowed to collect information from both sides of the contact line, and its data, while incomplete, remains the best available.


The OSCE observer mission provides maps in daily reports documenting the location of ceasefire violations and explosions along the contact line between the Ukrainian military and the Donbas republics.
These maps clearly show that Ukraine began artillery strikes against the Donbas republics on February 16th, 2022.
In other words, Ukraine began shelling the independent republics of Donetsk and Luhansk nine days before Russia announced its ‘special military operation’ in Ukraine.
While the western corporate media remained completely silent, explosions documented by the OSCE increased from 76 on February 15th, to 316 on February 16th, to 654 on February 17th, and to 1,413 on February 18th.
When you look carefully at the daily maps of these explosions, it is clear that the vast majority of explosions occurred on the Russian separatist side of the ceasefire line.
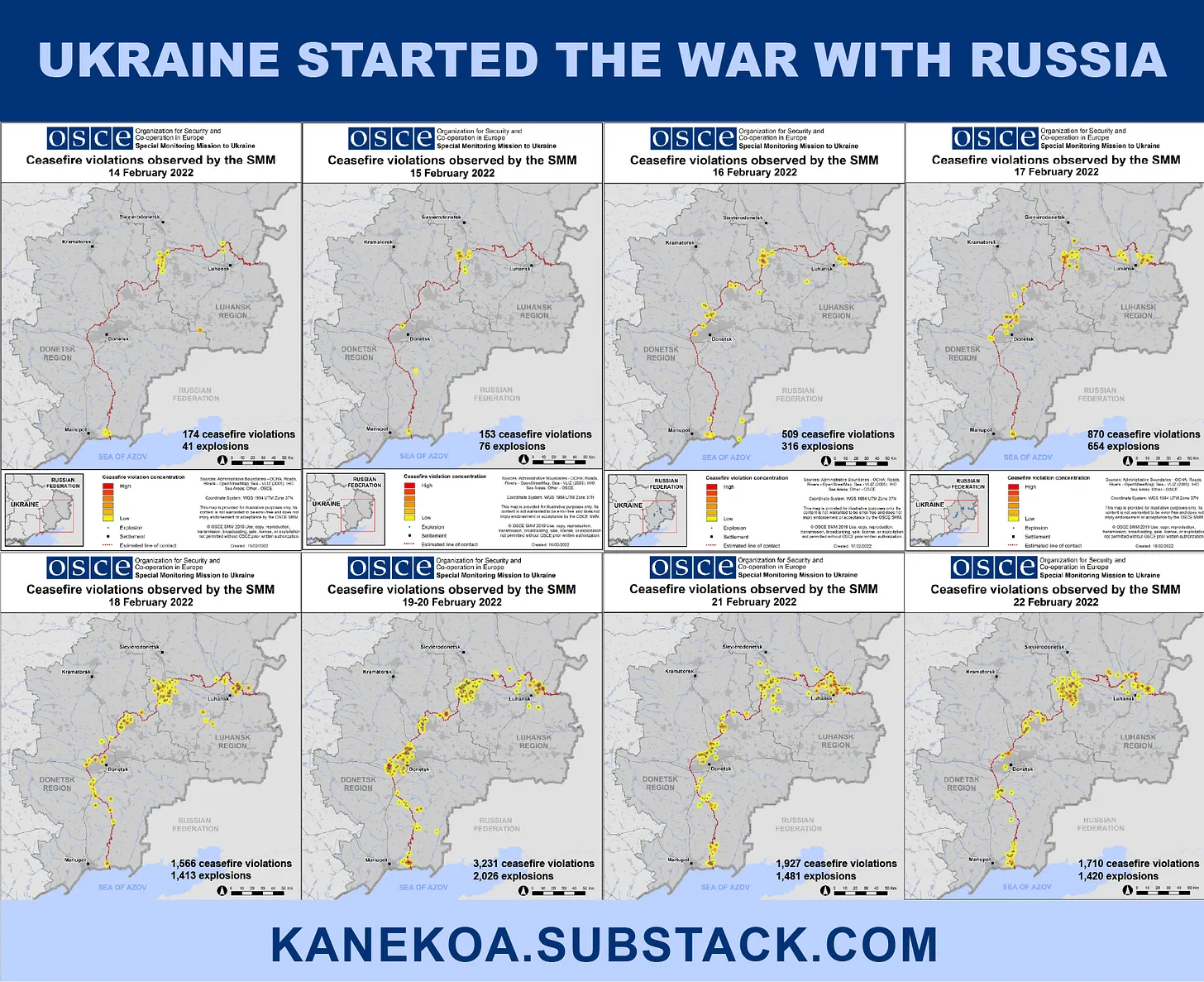
Feb 14: 174 ceasefire violations, 41 explosions
Feb 15: 153 ceasefire violations, 76 explosions
Feb 16: 509 ceasefire violations, 316 explosions
Feb 17: 870 ceasefire violations, 654 explosions
Feb 18: 1,566 ceasefire violations, 1,413 explosions
Feb 19-20: 3,231 ceasefire violations, 2,026 explosions
Feb 21: 1,927 ceasefire violations, 1,481 explosions
Feb 21: Russia recognizes independence of Donetsk and Luhansk
Feb 22: 1,710 ceasefire violations, 1,420 explosions
Feb 24: Russia launches ‘special military operation’

Jacques Baud, a former NATO intelligence analyst wrote about the OSCE reports, “On 17 February, President Joe Biden announced that Russia would attack Ukraine in the next few days. How did he know this? It is a mystery. But since the 16th, the artillery shelling of the population of Donbas had increased dramatically, as the daily reports of the OSCE observers show.”
While the western media spent the last year reporting on Russia’s troop buildup at the Ukrainian border, they failed to inform the public about Ukraine amassing “half of it’s army or 125,000 troops” along the Donbas conflict zone during this same time period.
Ukraine began to reposition its forces along the Donbas as early as March 24, 2021, when Volodymyr Zelensky issued a decree for the recapture of the Crimea, and began to deploy his forces to the south of the country.
It is unlikely Zelensky would make such an aggressive decree without first receiving the approval of the United States and NATO.
In April 2021, the Ukrainian government publicly announced that they would seek nuclear weapons if they were not issued membership in NATO.
This further signified that Ukraine intended to cross Vladimir Putin’s line in the sand by either joining NATO or placing nuclear weapons on Russia’s doorstep.
In that same month, Russia’s Defense Minister Sergey Shoygu accused the U.S. and NATO of moving troops to Russia’s borders.
“In Poland and the Baltic states, US forces are being reinforced … the intensity of aerial reconnaissance has been doubled compared to last year, and the intensity of naval reconnaissance has increased by one-and-a-half times,” he said.
The minister accused the US and its allies of carrying out active military activities “with a clear anti-Russian orientation”.
“In the spring of this year, the joint armed forces of NATO began the largest exercise in the last 30 years, Defender Europe 2021,” he said.
While both sides accuse the other side of being the aggressor, the OSCE maps clearly show that the Ukrainian side backed by the United States and NATO forces began shelling the Russian side on February 16th, 2022.
This shelling is corroborated by on-the-ground video journalism from an independent reporter named Patrick Lancaster who has been interviewing civilians in the eastern Ukrainian warzone for the last eight years.


On February 17th 2022, Lancaster reported on the increased shelling coming from the Ukrainian side and interviewed residents living along the contact line in the Donetsk region.
On February 19th, Lancaster reported on the Ukrainian military shelling two power plants knocking out electricity for multiple villages in Donetsk.
Ukraine Attacking Infrastructure Of Anti Ukraine Government DPR.
Patrick Lancaster
On February 20th, Lancaster interviewed residents of two homes that were attacked by Ukrainian mortar shells.
On February 21st, Lancaster visited two schools attacked by Ukrainian shells in the Petrovsky district of Donetsk.
Lancaster interviewed a female teacher cleaning broken glass from the shattered windows who said, “It is not the first time, it is the second time this school has faced a horrible attack! How do we teach children after that, tell us? Don’t you dare say that the Donetsk People’s Republic are shelling themselves! It is a nightmare, it is horrible!
She continued, “Ukrainians say that they do not shell civilians — then who shelled here? Here’s a direct hit from the Maryanka district, exactly where they stand. It is visible where it flies from. We do not sleep for 3 nights already. It is horrible, it is a shock, how is it possible? They are shelling their own brothers, sisters, and children!”
https://www.youtube.com/watch?v=cFl2IDsHsYk
A 23-year-old television producer who worked at the television network explained that the Ukrainian side was targeting journalist or those who “spread the truth about the events in Donbas” because the “information war” had gotten so serious that it now involved “the physical elimination of journalist.”
 / patricklancasternewstoday
/ patricklancasternewstoday
 / plnewstoday
/ plnewstoday
 / plnewstoday
https://t.me/patricklancasternewstoday
Patrick Is only funded by his viewers so please donate to help him continue his work.
https://www.youtube.com/watch?v=aSimLXmcmWw
/ plnewstoday
https://t.me/patricklancasternewstoday
Patrick Is only funded by his viewers so please donate to help him continue his work.
https://www.youtube.com/watch?v=aSimLXmcmWw
In summary, the Biden administration and U.S. political officials with the help of the corporate media are once again lying the public into another war based on false pretenses.
The OSCE reports and Patrick Lancaster’s on-the-ground reporting clearly show that Ukraine began shelling the independent republics of Donetsk and Luhansk nine days before Russia announced its ‘special military operation’ in Ukraine.
The same discredited neoconservative and neoliberal establishment that lied about Iraq, Afghanistan, Syria, and Libya are once again lying about Russia and Ukraine.
A diplomatic solution with Russia might have involved something as simple as demilitarization of Ukraine and a signed treaty promising Ukraine would never join NATO, but the U.S. political establishment wanted this hot proxy war with nuclear-armed Russia so they created it.
Ukraine started shelling the Russian-speaking people of the Donbas on February 16th, 2022, while Joe Biden went on television and told the American people that Russia was about to invade Ukraine.
You can find me on telegram, rumble, gab, and truth social.
Subscribe to Kanekoa News
REPOSTED FROM:
https://www.kanekoa.news/p/osce-reports-reveal-ukraine-started
___
eof